The Truth About Healthcare
Your daughter’s 103-degree fever sends you to the ER at 2AM. Three hours and some Tylenol later, you’re sent home, to confront with a bill for $1,847. Oh, and that’s just the specialist. That doesn’t include the separate $1280 “Emergency Room Services fee”!
Worse, your insurance denies coverage for the medication your doctor prescribed and suddenly you’re facing financial ruin to restore your health. This is American healthcare. Medical debt is the leading cause of personal bankruptcy in the United States, and nearly half of American adults have delayed or skipped care because they couldn’t afford it.
Healthcare needs a reset because our healthcare system is designed to be expensive.
Where Your Healthcare Dollars Actually Go
While your doctor may claim that every procedure is necessary, and that every cost is accounted for, the reality is, there’s a great deal of inflated pricing, bureaucratic padding, and waste.

Health Systems Stiff Patients
Every visit to the doctor, every test, procedure, and prescription costs FAR more than it should. How do they get away with that? They join health networks. When hospitals merge and form large health systems, they gain the power to charge whatever they want. Here’s what the research shows:
93% – Of hospital mergers led to higher prices
13% – Higher prices charged by system-affiliated hospitals vs. independent hospitals
22% – Of mergers showed ANY improvement in quality or cost
💡 Think of it this way: If our local grocery stores merged and raised prices, the law would prosecute them as a CARTEL. But that’s how hospitals are operating.
Prescription Drug Prices Are Out of Control
Americans pay dramatically more for prescription drugs than people in other wealthy countries:
All Drugs in U.S.: 2.78x higher than other countries
Brand-Name Drugs: 3.22x higher than other countries
Pharmacy Benefit Managers (PBMs), the middlemen between drug companies, pharmacies, and your insurance, should be able to lower lowering costs. Instead, they:
- Keep secret profits through “spread pricing” (charging your insurance $100 for a drug they pay the pharmacy $80 for)
- Don’t pass negotiated savings to patients
- Control 67% of the market through just four companies
For this reason, in October 2025, President Donald Trump cut a deal to lower prescription drug prices in the United States. Under the agreement, Pfizer will charge Medicaid the lowest price it offers in other developed nations—referred to as “most-favored-nation pricing”—and extend this pricing to newly launched drugs for Medicare, Medicaid, and commercial payers. Good on Trump, but that’s only a start.
Cost-Shifting Drives Insurance Up
Government insurance programs (Medicare and Medicaid) don’t reimburse hospitals enough to cover their actual costs. Hospitals get 82¢ on the dollar for Medicare, forcing some hospitals to reject Medicare, and others to charge private insurance companies more to make up the difference. And what a difference! $99.2 Billion Shortfall
💰 The Result: If you have insurance through your job, your premiums are higher because you’re subsidizing everyone on Medicare and Medicaid.
Insurance Paperwork Costs Billions
Hospitals spend more than 40% of their budgets dealing with insurance companies—getting approval for treatments, fighting claim denials, and managing billing.
20% – Increase in commercial insurance denials (2022-2023)
56% – Increase in Medicare Advantage denials (2022-2023)
🔄 Insurance companies create more hoops to avoid paying claims, so hospitals hire more staff to jump through those hoops. All this paperwork translates into more expensive premiums and medical bills.
Defensive Medicine: Why Doctors Order Tests
Never confuse diagnosis with treatment. When doctors push for more tests, in many cases, they’re not trying to be thorough. They’re trying to protect themselves from lawsuits. Ambulance chasers make $ millions off a wrong diagnosis, so doctors’ “CYA” covers their liability (and help pay for expensive tools).
But “defensive medicine” costs the system up to $50 billion per year.
Your PCP Is a Referral Dealer
While a “Value-based care” system rewards healthier patients through prevention, effective coordination, and positive outcomes, our current “Fee-for-Service rewards Primary Care Physicians for handing out more tests visits, and REFERRALS to specialists.
Obamacare Was Never The Affordable Care Act
The left claims the ACA provided affordable insurance to “millions of uninsured” since it reduced the number of patients with NO insurance. They never calculated the perverse incentives. Or the cost. Yes, you lost your doctor and plans, and drove millions under a Medicare umbrella while driving hospital systems off Medicare. Oh yeah, its rules drove insurance companies to raise premiums, and reduced incentives to fight pricing too.
After all, providers can simply pass on extra costs onto YOU, the consumer. And you get to pay into a system that rewards deadbeats, refuses to punish illegals, and never considers why the costs keep going up.
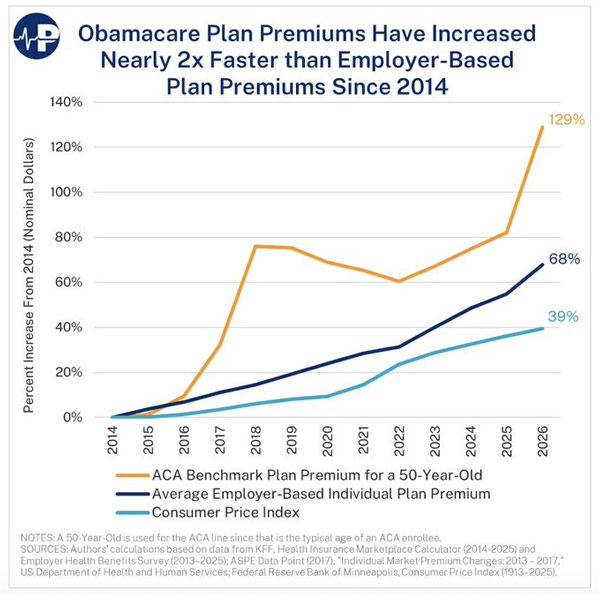
In 2025, average premiums for ACA plans rose 18 percent —the largest since 2017 — as all the tax gimmicks thrown into the cauldron expire, exposing the inherent problems Conservatives have been screaming about since Obamacare’s inception.
And we all know by now the truth: Obamacare was never supposed to work. It was designed to fail so that big government elites could usher in “single-payer” universal healthcare run by the DMV. Costs will then be standardized, doctors will flee to Wall Street to cover their insurmountable student debts, and Death Panels will decide whether you get rationed care or get offered the more affordable option.
How to Reset Healthcare 🎯
Before brainstorming a quality healthcare environment that is sustainable, affordable, and successful, we must come to grips with a few basic tenets:
- Forget Band-aid solutions. I have NO interest in “saving” a decrepit, institutionalized, unworkable systems so some politicians can save face and continue taking kickbacks from Big Pharma.
- Any option that gives GOVERNMENT more power is the WRONG idea. Our government has proven itself incapable of controlling costs, innovating, and providing effective service and incentives.
- Our solutions must empower the CITIZEN toward wholistic, thriving health, and longevity, not merely another strategy to treat symptoms.
In other words, we don’t exist to feed Pharma’s profits. We the People are sovereign and want to lead long and happy lives. We expect that our government, industries, and institutions should serve us.
Most central planners and healthcare policy makers immediately search for more top-down, government based, of government directed, strategies designed to keep existing services intact (and lobbying perks coming!) while tossing crumbs to the poor and disadvantaged.
That’s not where we should start. Instead, what are the individual obstacles to care? Consider that first step into the Emergency Room. What do we face?
Security. Paperwork, several screens or pages involving lists of rare disorders, family histories, and all your insurance details. Then waiting, sometimes for hours until we’re taken to a room where a nurse takes down “vitals” and then asks us to wait again for the doctor!
Screw all that. We’re now 3+ hours into a $1000+ fee and nobody is even triaging why we’re there!
Begin with Patient Empowerment and Innovation
Walk this idea around: Health Administration portal. Imagine the cross between Google and American Express (privately held preferably) providing Health Service Cards (like a credit card) with online storage to contain ALL our health related information. For all I know, it may already exist.
WAIT!! Isn’t that what Clinton offered back before The Contract for America “ended the era of big government?”
No. In this scenario, the Government doesn’t own your health access. You doctor doesn’t own or store your health data. YOU DO. This is your PERSONAL health account. You don’t ask doctors to send sets of X-rays or whatever, YOU store all that data in the cloud and you GRANT TEMPORARY ACCESS to service providers.

You control your data, family history, eating and exercise habits and such. You enter and maintain your health insurance data and set biometric scans (fingerprint or eyeball) as both password and proof of identity.
That means when you walk into a hospital, slip the Health Services Card into a Kiosk that reads your card and scans your identity, and AI asks for your symptoms (Yes, today’s technology). You enter your symptoms and the AI analyzes your health history, compares it to every recorded health case in the last 100 years, and makes a diagnosis to YOU and first level support – a NURSE. The nurse can take “vitals” if necessary (probably not) and either resolves the issue, or routes you to a doctor. That is, until those Star Trek tricorders come online.
In other words, our 3+ hour ER waiting ordeal is down to an under 2-minute AI-prompt. This not only accelerates AI adoption in healthcare, it also shifts control to the PATIENT. Remember, this is YOUR HEALTH. Not their CYA.
Depending on the situation, we may only need a human to rubber stamp the obvious treatment. Or at least when the doctor enters, he has ALL relevant data at his fingertips and can reassess, debate tests and treatment options with you, or simply practice his bedside manner.
And the cost? Almost nothing. Today’s AI models with minimal prompt engineering can get us most of the way. And with virtual healthcare taking off, going to the ER would be fast, and mostly reserved for serious cases.
How would this Health Administration company make money?
Just as Google sells our online search data, this company would profit by selling reams of medical data for analysis and product development. It would quickly fund all those free cards and data content (like Google drive), and the research from all this data might accelerate medical breakthroughs.
And YOU decide how much data from your account is accessible by whom for what. That means you can grant pre-access to local providers, set up exercise and diet campaigns (with AI encouragement), and request product types in an online health marketplace.
Sounds like a capitalist paradise, eh? It won’t be perfect but it’s better than rationed care and death panels.
Want to glimpse what the future could look like? Check out new start-ups like Superpower.
Reset Insurance to Prevent Bankruptcy
The Eisenhower and Nixon administrations developed and expanded employer-sponsored insurance (ESI) by allowing employers and employees to exclude health benefits from taxable income. It required all employers to offer health insurance to full-time employees, with premiums shared between employers and employees. This pushed more working Americans into the private insurance market rather than the alternative: a government-run single-payer system.
Obamacare changed that. It’s a government TAX (thanks, SCOTUS!) compelling Americans into a private service through a confusing, convoluted (and [cough] unconstitutional!) exchange. While it feels like another wealth redistribution ploy, it serves to drag us toward “universal healthcare” where our taxes skyrocket while healthcare quality plummets.

Insurance was invented to prevent disaster from bankrupting families. That’s why we have car insurance. Homeowner’s insurance. And yes, health insurance… Except that policy makers then thought it should also cover basic checkups, and kept heaping other responsibilities on it until it became like a single-payer system. Well, except what government program (Medicare/Medicaid, Plus, etc blah blah) determines it won’t fund, and what your insurance won’t cover.
Let’s go back to its original intent: as a bankruptcy backstop. Insurance should be cheap and reasonable, and kept from almost ALL healthcare related decisions since it’s none of their business.
We should also move to decouple insurance from employment. Each time employers switch insurance providers to find a better deal, “preexisting conditions” come into play, and employees get shafted with larger premiums and/or copays.
The laws should be modified so that “pre-taxed employer contributions” become UNtaxed employer contributions that go directly into personal Heath Administration accounts. That allows WE the PEOPLE to choose our providers.
If insurance groups are still needed to spread the wealth (a-hem?), insurance policies should target by geography, age, condition or whatever. That way we incentivize better behavior and lifestyle choices, and then “if you like your doctor you can keep your doctor” when you change jobs in a world where workers tend to change jobs.
The obvious result is less paperwork for doctors, and citizens have faster service and less hassle. Ta-da!
But Isn’t There a Role for Government in Healthcare?
This question presupposes government SHOULD have a role in healthcare! WHY?!!!
The real question is, how do we incentivize healthcare to innovate, become CHEAPER and BETTER. The current public policies incentivize doctors, hospital systems and Big Pharma to treat symptoms instead of find cures. It infantilizes citizens, uses taxes to punish the uninsured in other to patronize the “helpless” poor!
Once we establish a system that lowers healthcare costs, we’ll see clear how to solve helping the poor.
To that end, government should make policies to stop “The money is in the meds,” because pharma-based healthcare is evil. Pharma lobbies government for favorable tax treatment and designs pills that mask symptoms and pacify us. It’s a system that empowers the very institutions that have made us sicker, weaker, and poorer, for decades.
I realize AI is no panacea but it’s a LOT closer to our more perfect union because it doesn’t have an inherent profit motive. It could be programmed to run lifestyle modification scenarios. It also links up well with other innovations like wearables, medbeds, nanotech, and the like. it’s an amazing time to be alive provided the solutions we create aren’t used to impoverish the citizenry.
Where Do We Start?
We’ve just scratched the surface. Whole industries are wrestling with heath innovations and strategies. The new rich, like Bryan Johnson, are trying to anti-age, and their exploration could discover new worlds of health for humanity.
The Make America Healthy Again (MAHA) movement has already beaten concessions out of Pfizer to lower drug prices for Americans, and several manufacturers to remove cancerous food coloring. I can’t wait for more developments as RFK Jr. gets to the bottom of the COVID poisons, and the underlying causes of autism related to vaccines and other sacred cows government and the health industry have hid from us.
For most of us, it means taking small Kaizen steps in the right direction. Where to start?
- Ask small questions: If my health was a top priority, what would I do differently? How healthy are the foods I love to eat? Am I overweight? What are my exercise habits, if any?
- Think small thoughts to develop new skills and habits: Wait, is my PCP just a referral dealer or can he recommend a strategy that doesn’t cost me a bundle? Is Creatine right for me?
- Take small actions that guarantee success: I’m going to replace one sugary snack with fruit. I’m going to switch from chips to protein.
- Solve small problems: Put together a family health record to be ready when the time comes. Document your relationship with your Insurance provider.
- Bestow small rewards to yourself or others to produce the best results: If I walk a mile today, I’ll reward myself with another piece of fruit. It’s better than that sugar thing anyway.
- Recognize the small but crucial moments that everyone else ignores: Start a dinner conversation about the time we became a health-conscious family. Or can we start now?
What do you think?
How can you add to the cultural conversation? No, I don’t believe like Tyler Durden that “All self-improvement is masturbation” or that our healthcare is too far gone. We’re not doomed. We will NOT go quiet into that good night!
If that’s you, what’s your plan?
Stay in Touch
Reducing the impact of leftism, statism, and other negative influences can be difficult. Let’s do it together.
If you have suggestions for resetting our cultural conversation, or just want to be kept up-to-date, send me a question or comment.
Reset Culture